


 Copy to clipboard
Copy to clipboard 
Knee and hip preservation are emerging as a significant trend in orthopedics, driven by the need to treat younger, more active patients who aren’t yet interested in joint replacement surgery.
For patients undergoing partial knee resurfacing, replicating the function of native cartilage has been a barrier to successful outcomes. Hip resurfacing preserves bone and maintains more natural joint biomechanics but concerns about metal-on-metal wear debris has limited its adoption.
Those challenges are being addressed with advances in materials science and implant design that allow for the development of devices that better maintain native anatomy and restore joint function, delaying the need for more aggressive treatment options.
Engineering Synthetic Knee Cartilage
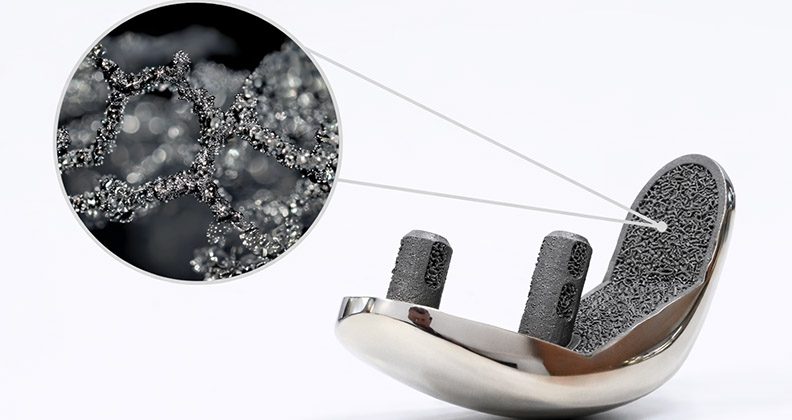
BioPoly’s Partial Resurfacing Knee Implant combines ultra-high-molecular-weight polyethylene (UHMWPE) with hyaluronic acid (HA).
“The key to the BioPoly material lies in the combination of UHMWPE and HA, which produces a hydrophilic polymer that is ideal for orthopedic applications,” said Herb Schwartz, Ph.D., CEO, President and Founder of BioPoly. “UHMWPE provides the structural backbone, carrying anatomic loads with mechanical properties that meet the same ASTM standards required for total joint materials. HA, meanwhile, fundamentally changes how the material behaves in the joint environment.”
HA imparts hydrophilic properties on the polyethylene, allowing BioPoly to attract surrounding synovial fluid to its surface for use as lubrication, just like cartilage does, according to Schwartz.
BioPoly therefore replicates the function of cartilage, not necessarily its mechanical properties. That distinction is critically important, Schwartz noted.
As a biomechanical engineer, Schwartz has seen repeated attempts to match cartilage’s mechanical properties with synthetic materials. In his view, that approach doesn’t address the biology of the knee joint.
“Native cartilage survives because it can regenerate its matrix through living cells, which is something a synthetic implant cannot do,” he said. “If you match the mechanical properties of cartilage with a synthetic, nonregenerative material, the synthetic material will fail over time in a real joint environment.”
Instead, BioPoly maintains the durability and elasticity of UHMWPE while using lubrication, not material softness, to protect native cartilage. The result is a surface that glides rather than grinds, even under high loads and constant motion, to minimize contact with cartilage and reduce wear.
That material behavior becomes especially important in partial resurfacing applications, where the implant must coexist with native cartilage on multiple fronts. BioPoly interfaces with opposing cartilage during articulation, adjacent cartilage at the implant margins and subchondral bone beneath the joint surface.
Each of these functions presents unique engineering challenges.
While BioPoly’s modulus is slightly higher than cartilage, it is far lower than cobalt chrome or metallic implants, reducing the risk of localized overload. Surgical instrumentation and technique also account for these differences, ensuring the implant sits appropriately relative to surrounding cartilage.
According to Schwartz, an implant’s long-term integration with adjacent cartilage is also a critical component of its design. To that end, BioPoly exhibits a unique biological response after implantation.
Chondrocytes attach themselves to the material, allowing surrounding cartilage to seal to the implant over time. “This sealing effect is especially important in the knee, helping maintain joint fluid within the articulation and preventing fluid intrusion into the subchondral bone,” Schwartz said.
Below the surface, fixation to bone is achieved using titanium stems selected for their biocompatibility and elastic modulus. The subchondral bone bonds to BioPoly’s engineered titanium surface, providing durable fixation that has been validated clinically.
BioPoly has published two- and five-year knee results in The Journal of Bone and Joint Surgery, providing long-term data that supports implant stability and bone health.
The material’s clinical performance is being evaluated in an FDA-approved randomized controlled IDE trial underway in the U.S. The trial focuses on patient-centered endpoints such as pain reduction and short- and long-term quality-of-life improvement.
BioPoly’s partial resurfacing knee received CE Mark in 2012, and the company has successfully brought its patella and trochlea implants to market outside of the U.S., as well as received FDA 510(k) clearance for its Great Toe System, Lesser Toe System and Radial Head Implant.
Manufacturing the synthetic cartilage implant presents its own complexities. Schwartz said combining UHMWPE and HA is like mixing oil and water. Years of proprietary chemistry development were required to create a consistent, scalable process.
Today, the Biopoly material matches the strength of traditional UHMWPE without damaging cartilage over the long term. Final implants are produced using direct compression molding, a process well-suited for scale.
Ceramic Hip Resurfacing
MatOrtho’s ReCerf is the first commercially available all-ceramic hip resurfacing system.
The system is based on BIOLOX delta ceramic, a material with decades of clinical use in total hip arthroplasty. According to Danielle de Villiers, Hip Manager at MatOrtho, that proven history made ceramic a natural choice for resurfacing if it could meet the unique demands of a thinner, larger-diameter implant.
“BIOLOX delta ceramic was the right material given its long and successful clinical history in total hip replacement,” de Villiers said. “The material has shown to be low wearing and biocompatible while reducing the risks surrounding fracture, which had been prevalent in previous generations of ceramics.
“We knew the material already worked in orthopedics, and that gave us more confidence in applying it to a hip resurfacing design that we knew worked from our history with the Adept metal-on-metal hip resurfacing.”
Transitioning from metal-on-metal to ceramic-on-ceramic directly addresses the issues that constrained earlier resurfacing systems.
Wear debris and adverse biological reactions were central to concerns around metal-on-metal hip resurfacing. By replacing metal entirely, ReCerf eliminates those risks while retaining the core biomechanical advantages of resurfacing.
“The ceramic articulation removes the metal from the device,” de Villiers said. “Ceramics are lower wearing and biocompatible, which addresses these issues.”
Just as importantly, ceramic has enabled MatOrtho to expand resurfacing to a broader patient population.
“Metal-on-metal devices were limited in sizes and predominantly used to treat men,” de Villiers said. “The ceramic has allowed us to expand the applications of ReCerf, and clinical evidence out to seven years is demonstrating that ceramic-on-ceramic can successfully be used in female patients and in smaller sizes.”
Material behavior becomes even more critical in hip resurfacing because bearing diameters are larger than those used in total hip replacements. Low wear is essential, as is resistance to fracture in a thinner geometry.
“As hip resurfacing devices have larger bearing diameters than total hip replacements, the wear behavior of the material is critical,” de Villiers notes.
Ceramic-on-ceramic allows for a hard-on-hard articulation that produces lower wear rates than hard-on-soft bearings. Achieving the low-wear behavior, however, requires precise control of surface finish and clearance.
“The design of a hip resurfacing is often thinner than a total hip replacement femoral head or acetabular liner and so the fracture resistance of the material is also a key consideration,” de Villiers said.
Applying ceramic materials to a resurfacing geometry requires substantial engineering and manufacturing development. While BIOLOX delta had a long track record in total hip replacement, ReCerf demanded larger diameters and thinner components than what was traditionally manufactured.
“We conducted extensive development and testing with CeramTec to ensure the material would withstand clinical conditions up to forces where the native bone would break,” de Villiers said.
These tests and rigorous validation addressed common concerns about the brittle nature of ceramic components.
Beyond materials and manufacturing, ReCerf is designed to preserve native anatomy while providing stability and durability for active patients.
The femoral component functions as a cap placed over the native femoral head, preserving the femoral neck and maintaining the natural diameter of the joint. This design feature creates a larger bearing surface than total hip replacement and allows the hip capsule to remain filled, allowing for greater stability and range of motion.
ReCerf’s acetabular cup is monobloc, which eliminates the need for a separate shell and liner. At just 3mm thick, it preserves bone while removing the risk of liner/shell dissociation.
From a biomechanical standpoint, hip resurfacing offers a fundamentally different approach than total hip arthroplasty.
“Hip resurfacing aims to restore the patient’s anatomy by maintaining the native diameter of the femur and preserving bone,” de Villiers said.
The benefits of closely replicating the hip’s natural mechanics are most apparent during demanding conditions such as fast walking, hill climbing and running. Retaining the femoral neck bone is a crucial part of this design concept from a biomechanical perspective.
For MatOrtho, ReCerf also reflects a broader philosophy of innovation.
“We believe in careful and stepwise innovation, which we have achieved with ReCerf by not altering too many aspects of the design and material in one iteration,” de Villiers said. “This lesson will continue to inform the development of our next generation of devices.”