Copy to clipboard
Copy to clipboard 
For proof that regenerative medicine is going mainstream, look no further than the MMA cage where fighter Ryan Cafaro recently stood victorious 11 months after undergoing surgery to treat his torn ACL.
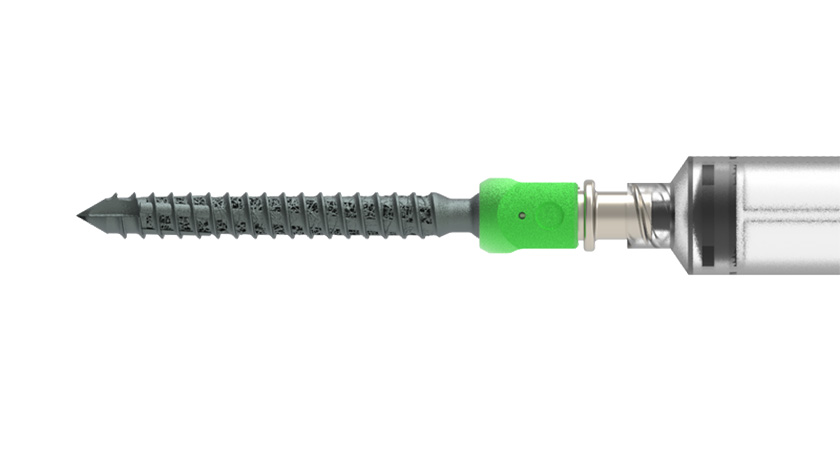
During the post-match interview, Cafaro didn’t thank his trainer, his family or even a higher power. He instead shouted out Sean McMillan, M.D., a sports medicine specialist in Philadelphia, for inserting the BEAR implant in his knee. The novel device bridges the gap between the edges of an ACL tear, allowing the ligament to repair itself over time.
The BEAR implant, manufactured by Miach Orthopedics, counteracts the presence of synovial fluid, which prevents the ACL from forming a stable clot that promotes healing. During a minimally invasive surgery, surgeons inject a small amount of the patient’s own blood into the implant and insert it between the torn ends of the ACL. The implant holds and protects the patient’s blood, allowing a clot to form.
Orthopedics has been somewhat slow to embrace biological solutions like the BEAR implant. Our market analysis shows that all players in the segment hold less than 10% of the market share, and companies that generate less than $50 million in annual sales make up 44% of the market. That dynamic might change as more established companies and startups invest in the largely untapped market.
“Recent acquisitions in the sports medicine space have shown that regenerative medicine is becoming more of a priority,” said Patrick McBrayer, President and CEO of Miach Orthopedics. “While there are only so many ways to create rods, screws and plates, biologics offer the ability to create new treatment options.”
Restoring Form and Function
FDA granted Miach Orthopedics its De Novo request for the BEAR implant, a significant development in the sports medicine space. The implant is the only available technology that restores a patient’s native ACL without disrupting the knee’s natural mechanics. Surgeons are not required to perform a second surgical procedure to harvest a healthy tendon from another part of the patient’s leg or worry about managing and implanting donor tissue.
Eliminating the need to harvest autograft implants or transplant allograft tissue results in significant workflow advantages. It also provides significant clinical benefit. Removing hamstring tissue to repair the ACL disrupts the muscle’s strength symmetry and can have a lasting impact, according to McBrayer. “Surgeons rob Peter to pay Paul by disrupting native anatomy when they harvest autograft tissue,” he said.
Reconstructing and restoring the ACL are two distinctly different ways of treating tears. The latter approach is garnering significant interest in the sports medicine segment.
“A reconstruction is never going to reestablish the knee’s natural form,” said Arjun Ishwar, Vice President of Sales and Marketing at Miach Orthopedics. “The BEAR implant aims to do both by providing a scaffold that allows surgeons to induce the formation of a healing clot. It helps to restore the knee’s natural form, which restores its natural function.”
Focusing on Fracture Repair
Surgeons love to heal with steel. The current standard of care for tibia fractures involves placing an intramedullary rod and waiting for the body to mend the fracture, which takes nine to 12 months. “This is problematic for several reasons, including the high cost of imaging, doctor visits and rehabilitation, as well as the negative impact on quality of life and work productivity,” said Randy Hubbell, CEO of Carmell Therapeutics. “Additionally, comorbidities such as obesity, smoking, diabetes and aging can inhibit tissue repair and bone regrowth.”
The company received FDA’s Fast Track designation for use of its Bone Healing Accelerant (BHA) in tibia fracture healing. The company has completed a phase 2 trial of the product and is expected to enroll the first patient in a clinical trial in 2Q23.
The BHA is a mixture of plasma-based bioactive material and beta-tricalcium phosphate, which is commonly used for bone growth. It’s made from allogeneic platelet-rich whole plasma, which guarantees a high level of bioactivity by eliminating units that do not meet the platelet threshold. It contains multiple growth factors, including PDGF, VEGF, IgM and EGF.
“This results in a higher average platelet count than what individuals can produce on their own with autologous PRP,” Hubbell explained. “The high level of bioactivity is significant because it can signal cells to proliferate, migrate and differentiate in bone regrowth. That’s crucial for proper bone healing.”
The product accelerates the healing process in normal and compromised environments, according to Hubbell. “By reducing the healing time from 12 to six months, we can significantly reduce downstream costs and improve patients’ quality of life,” he said. “While other products provide scaffolding for bone regrowth, they may not have the necessary growth factors to properly stimulate cell activity.”
Hubbell also pointed to the off-the-shelf application of the BHA as one of its significant benefits and an important aspect of its development. “Introducing technology that adds steps to established surgical workflows can result in unattended consequences that may or may not be related to the new product,” he said. “Ease of use is critical to adoption and to ensuring it’s used correctly, which is important from an outcomes perspective.”
Carmell Therapeutics is currently going through the regulatory process for Biologics License Application (BLA) approval — a rigorous pathway — because it wants to make claims about the bioactivity of the BHA’s material.
“Several well-controlled studies are important to show superiority over the standard of care, so hospitals know they’re buying a product that is not just substantially equivalent or non-inferior,” Hubbell said.
Carmell Therapeutics’ product pipeline consists of various applications in different stages of development. The company gained alignment with FDA on requirements to evaluate its BHA for a second indication: foot and ankle fusion surgery.
There is an unmet need for biologics in foot and ankle fusion, according to Hubbell. “AUGMENT bone graft is available, but it only contains one recombinant protein,” he said. “The hypothesis is that our BHA will have a greater clinical benefit, but we won’t know until we perform the clinical trials.”
FDA agreed that the company’s current IND of the BHA for tibia healing can be amended to allow for a phase II study on its foot and ankle application. The company also expects to complete a pre-clinical large animal study of a spinal fusion application in 3Q23.
Carmell Therapeutics’ BHA is representative of a larger trend in innovative approaches to helping the healing process.
“The future of regenerative medicine lies in allogeneic approaches, which do not require tissue or blood from the patient and instead use an off-the-shelf product that is guaranteed to be bioactive and produce meaningful clinical results,” Hubbell said. “This eliminates the need for procedures to obtain autologous material and allows for better control over the bioactivity of the product.”
Stem Cell Therapy Shows Promise
Fracture repair is a complex process that is often oversimplified in the orthopedic community as an injury involving a bone that will reform and heal, according to Philipp Leucht, M.D., Ph.D., Associate Professor of Orthopedic Surgery and Cell Biology at NYU Langone Health.
“In reality, fracture healing involves a sophisticated interplay of various growth factors that are exposed to different cell types and vary at every stage of the healing process,” he said.
This makes it difficult to design or translate human growth factors into biologics. For example, BMP-2 plays multiple roles in fracture healing, and its effects differ depending on when it’s administered. “Administering BMP-2 during surgery may cause an initial inflammatory response because the bone cells aren’t yet present,” Dr. Leucht said. “It’s essential to find the right growth factor and delivery method to ensure that it’s present at the right time and placed in the fracture for effective healing.”
A growth factor cocktail would be administered at specific time intervals and locations within the injury site to achieve maximum effectiveness, according to Dr. Leucht. But, he said, the maximum effect might not be necessary — a small amount of growth factor could be sufficient to kickstart the healing process, allowing the body to complete the rest of the repair.
“Some biologics already promote the early stages of repair, such as angiogenesis, stem cell division and blood vessel formation,” Dr. Leucht. “Stem cells present in a well-perfused fracture environment will deposit bone and initiate their healing process. This approach is more likely to be used in the future.”
Stem cells possess the ability to perform the same functions as biologics. “I’m excited by the potential of using stem cells for bone regeneration,” Dr. Leucht said. “Although surgeons must tailor their use of biologics to match the various stages of fracture repair, stem cells can respond appropriately to cues at repair sites and secrete growth factors to attract other stem cells that divide and deposit bone.”
The challenge is understanding how to increase the number of stem cells at the repair site, because insufficient numbers are typically the reason for poor bone regeneration. “If we can boost the number of stem cells, they will initiate the healing process if the right environment and signals are in place,” Dr. Leucht said.