Copy to clipboard
Copy to clipboard 
Craig McAllister, M.D., has witnessed firsthand the evolution of joint replacement surgery. First as a successful surgeon and owner of an ambulatory surgery center (ASC) and now as the CEO of Operativ, an orthopedic company based in Washington State that develops instrumentation for minimally invasive joint replacement techniques.
In the 1990s, his surgeon colleagues used to roll their eyes when he brought up the idea of sparing much of the knee’s natural anatomy when replacing diseased bone with metal implants.
“The prevailing approach back then involved making large incisions to accommodate bulky instruments,” Dr. McAllister said. “Patients typically stayed in the hospital for four to five days, needed blood transfusions and relied on heavy doses of narcotics for pain management. In many cases, procedures were so invasive that patients ended up in the ICU.”
Knee replacement surgery has evolved significantly since then with the improvement of soft tissue management, exposure methods and the incorporation of enabling technology. The procedure will never be likened to arthroscopy in terms of invasiveness, but these advancements have made same-day surgery a routine option.
The evolution of minimally invasive joint replacement surgery is indicative of a growing trend across all segments of orthopedics. Device designers and manufacturers are developing instruments, implants and enabling technologies that allow surgeons to perform surgery that results in less postoperative pain, fewer complications and faster recoveries. This trend is especially important as increasing numbers of orthopedic procedures are performed in ASCs.
Preserving Natural Anatomy
The various definitions of minimally invasive knee replacement surgery share a common thread: solutions that preserve the quadriceps muscle.
Dr. McAllister explained that traditional joint replacement surgery involves averting the extensor mechanism and patella. “Modern techniques have moved away from this approach with the development of soft tissue release methods, which allow surgeons to slide the patella over, similar to how they treat native patellar dislocations,” he said.
Minimally invasive techniques also involve a careful sequencing of bone cuts, eliminating the need to dislocate the tibia forward. “This used to be a primary step, which surgeons performed to significantly expand the surgical field,” Dr. McAllister said. “Today, they make some cuts in advance to decompress the soft tissue envelope.”
This allows today’s joint replacement surgeons to keep the knee within its anatomical envelope. “Instead of dislocating the patella and tibia to view the entire joint, surgeons approach the joint like keyhole surgery. They work in one part of the knee and then transition to another part,” Dr. McAllister explained. “The technique requires streamlined instruments with softened edges and smaller profiles.”
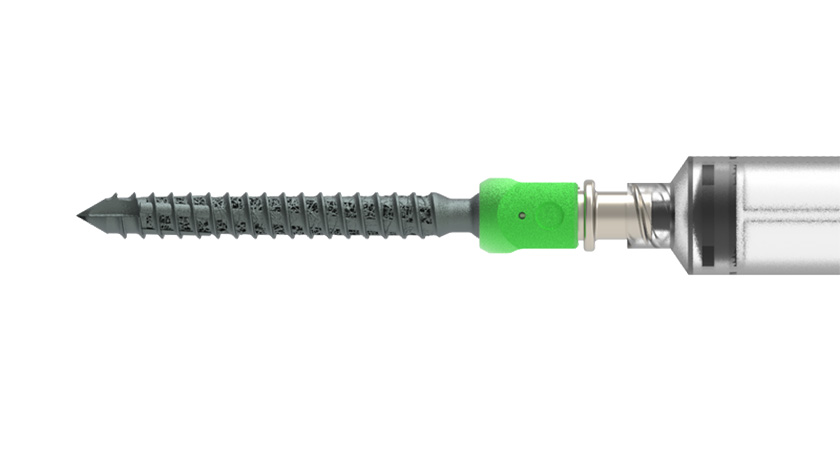
Dr. McAllister pointed out that surgeons once believed that large instruments were needed to ensure implants were precisely placed and joints were properly aligned. That’s no longer the case. His company has developed miniaturized instruments that communicate with navigation systems to support minimally invasive surgical techniques.
“We reevaluated conventional large instrumentation designed for an intrusive surgical approach,” Dr. McAllister said. “Our team made the tools smaller, rounded the edges and eliminated components needed for invasive surgery. The instruments are also about one-third the size of conventional designs.”
Operativ developed software and light-emitting diode (LED) transmitters that connect its instrumentation to navigation platforms. Surgeons attach transmitters to reference pins attached to the tibia, femur and ankle. The navigation system then calculates the location of the joint’s central position and uses the reference markers to create a digital recreation of the leg.
Attaching an LED transmitter to the cutting block allows the navigation system to calculate the block’s slope, varus/valgus angle and depth. This enables surgeons to use smaller, rounded cutting blocks and perform surgery with minimal joint exposure.
Although enabling technology has yet to gain widespread acceptance among joint replacement surgeons — robotics and navigation are used in about 20% and 11% of joint replacement cases, respectively, according to THE ORTHOPAEDIC INDUSTRY ANNUAL REPORT® published by ORTHOWORLD — those percentages are expected to increase as orthopedic companies invest in technologies that help to increase the precision of surgery.
“The literature is full of hard evidence that shows navigation improves knee replacement outcomes in terms of alignment, range of motion and ligament balance,” Dr. McAllister said.
Less Invasive Than Fusion
Spine companies are increasingly interested in developing minimally invasive surgical solutions.
Orthofix Medical recently announced the full commercial launch and first successful cases in the U.S. involving the 7D FLASH Navigation System Percutaneous Module 2.0. The system provides new planning features and increased functionality designed to provide surgeons with the information they need to perform more efficient minimally invasive spine surgery.
Viseon also recently began the U.S. commercial rollout of the MaxView 4K Advanced Visualization System for minimally invasive spine surgery. The towerless system takes up no floor space in the operating room, making it well-suited for use in an ASC. Jeffrey Valko, Viseon CEO, said that moving minimally invasive surgical techniques forward requires advanced visualization capabilities.
This March, Xtant Medical acquired the Coflex interlaminar stabilization device from Surgalign. The device is implanted after direct decompression surgery, offering a non-fusion treatment option for patients with lumbar spinal stenosis.
Coflex is a motion preservation device that is designed to preserve mobility, the natural flexion and extension of the lumbar spine. Clinical data shows the Coflex device provides superior stability and maintains the foraminal height compared to decompression alone, which further prevents collapse or re-stenosis.
“Motion preservation is incredibly important in the development of minimally invasive implants,” said Madeline Gonyea, Vice President of Payor Relations and Commercial Development at Xtant Medical. “It aims to preserve the range of motion of the spine at both the treated and adjacent segments.”
Patients with moderate to severe lumbar spinal stenosis traditionally undergo decompression alone or decompression combined with fusion. Gonyea said Coflex introduces a third option to the surgeon’s toolkit. After direct decompression, Coflex is placed in a laminar “landing zone” created by the surgeon where the implant matches the natural shape of the anatomy and preserves lordosis.
“The device supports controlled movement and provides stability after the surgeon has removed the obstructing anatomy,” Gonyea said.
Two prospective, randomized (Level 1) studies demonstrate better outcomes at specific time points for Coflex compared to fusion and decompression alone, according to Gonyea. She said direct decompression combined with interlaminar stabilization differentiates the use of Coflex from other treatment options.
“Positioning the implant near the instantaneous axis of rotation provides a better anchor point for natural biomechanical forces to occur compared to interspinous and plate devices which are often associated with spinous process fractures” she added.
Coflex is designed for motion preservation in the lumbar spine, a product category with relatively few options available. Gonyea said that it frequently gets lumped in with interspinous devices on the spine market, but believes it’s in its own product category.
“It’s implanted only after direct decompression and sits on the strong laminar bone, about 1-2 mm off the dura” she added. “The device fits a specific clinical need and cohort of patients who require more than a decompression but are not yet ready for a fusion.”
Supporting the Move to ASCs
Minimally invasive surgical techniques are increasing in importance as more cases move to ASCs.
Preserving much of the knee’s natural anatomy during joint replacement surgery allows patients to ambulate sooner and return home on the day of surgery. Smaller instruments and streamlined instrument sets that are designed for minimally invasive joint replacement techniques are easier for sterile processing teams at ASCs to reprocess and manage.
Dr. McAllister said one of the common criticisms of minimally invasive surgery is that the techniques take longer to perform. However, he argues that enabling technology makes procedures more efficient. Surgeons who use navigation and robotic systems know precisely where to make their cuts and don’t need to make adjustments at the end of the case to ensure the joint is properly aligned. Shaving minutes off operative times is a significant benefit in the outpatient setting.
Gonyea believes Coflex has a compelling value proposition for ASCs with established reimbursement codes. The device is supported by Category 1 CPT codes for single and second levels.
The device can be implanted midline between adjacent lamina of 1 or 2 contiguous lumbar segments, ranging from L1 to L5. If a procedure involves implanting Coflex, the ASC receives, on national average, $16,629. That’s about twice as much as the facility would receive for a standard laminectomy.
“This means that the product is not only great for patient outcomes, but it also has a positive impact on the facility’s bottom line,” Gonyea said.
The product is available in five sizes, ranging from eight to 16 millimeters in two-millimeter increments, to meet the anatomical needs of individual patients. Color coding distinguishes the five implant sizes, and product labeling clearly indicates the correct orientation for implantation. This ensures a smooth onboarding process for everyone involved in the procedure, from the scrub tech to the physician.
Coflex and the eight instruments needed to implant it — five size trials, wing bending plier, wing crimper and mallet — all of which come in a brownie-pan-sized instrument tray. “This compact instrument set simplifies the surgical process, which is appealing for ASC directors, who know that their sterile processing department won’t be overwhelmed,” Gonyea said.
Gonyea said Coflex is a slick solution that can reduce operating room time (compared to that of a fusion case), minimize blood loss and lower opioid usage during patient recoveries.
“That represents a substantial growth opportunity for the ASC,” Gonyea said. “We’re committed to educating not only surgeons but also ASC directors about the potential benefits.”